


" UNLOCKING THE MYSTERIES OF CHRONIC CORONARY SYNDROMES(CCS): A NEW ERA OF UNDERSTANDING AND TREATMENT "
(AN OVERVIEW OF ESC CCS 2024 GUIDELINES)
In 2019, the European Society of Cardiology (ESC) shook up the world of cardiology by redefining coronary artery disease (CAD) with the introduction of the term chronic coronary syndromes (CCS). This new framework broadens our view of CAD beyond just the blockages in arteries to encompass a wide array of conditions linked to the chronic health of the heart’s blood vessels. CCS now includes any issues related to structural or functional changes in the coronary arteries and microcirculation that can disrupt the heart’s blood supply, leading to symptoms such as angina, chest discomfort, or even asymptomatic conditions.
The evolution of our understanding of CCS has been dramatic. Previously, we thought of CAD primarily in terms of large, obstructive blockages in coronary arteries. Today, we know that CCS can also involve more subtle issues like diffuse atherosclerosis, coronary artery spasm, and coronary microvascular dysfunction (CMD). CMD, in particular, is now recognized as a major contributor to angina and ischaemia, even in patients who don’t have significant blockages in their large coronary arteries. These insights have expanded our view of what can cause heart-related symptoms and has led to more nuanced approaches to diagnosis and treatment.
CCS presents in diverse ways, depending on the underlying issues. Some patients experience classic angina due to blockages in the coronary arteries, while others may have symptoms from more complex conditions like microvascular dysfunction or vasospasm. There’s also a growing number of people who are asymptomatic but discover CAD through imaging tests done for other reasons. This variety means that CCS can be tricky to diagnose and treat, as symptoms can overlap with those of other heart conditions and vary by individual.
The approach to managing CCS has evolved alongside our growing understanding of the condition. Advances in prevention, such as lifestyle changes and new medications, have reduced the incidence of severe obstructive CAD. New diagnostic tools, including coronary computed tomography angiography (CCTA) and non-invasive imaging methods like PET and MRI, offer detailed insights into coronary health, helping clinicians better assess both major and minor issues affecting the heart. Invasive techniques like coronary angiography have also expanded to include assessments of coronary function and microvascular health.
Medical therapies for CCS have made significant strides, with improved antithrombotic, anti-inflammatory, and lipid-lowering treatments enhancing patient outcomes. Despite these advances, revascularization—such as percutaneous coronary intervention (PCI)—remains a crucial option for those with severe obstructive CAD. Recent studies have demonstrated that PCI can provide substantial relief from angina and prevent serious cardiac events, solidifying its role in the modern management of CCS.
As we continue to unravel the complexities of CCS, these advancements promise to offer more personalized and effective treatments, improving the quality of life for countless individuals living with coronary artery disease.
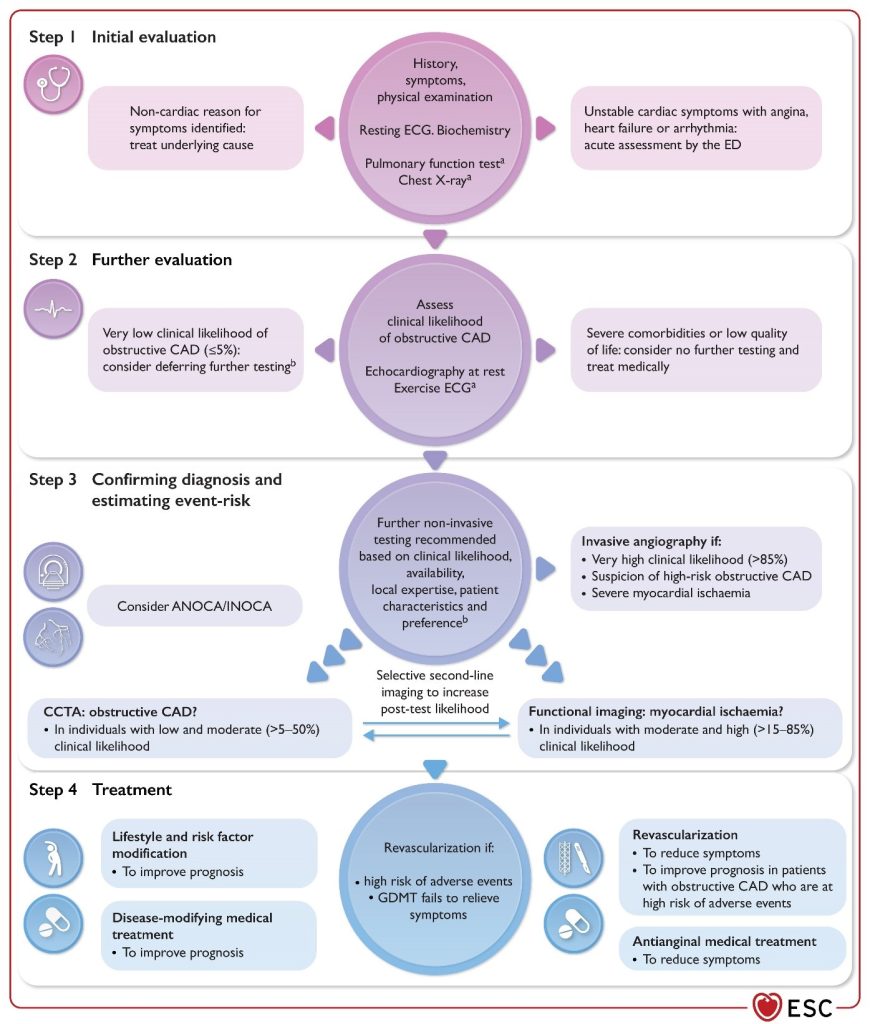
Figure 1
Stepwise approach to the initial management of individuals with suspected chronic coronary syndrome.
ANOCA, angina with non-obstructive coronary arteries; CAD, coronary artery disease; CCS, chronic coronary syndrome; CCTA, coronary computed tomography angiography; ECG, electrocardiogram; ED, emergency department; GDMT, guideline-directed medical therapy; INOCA, ischaemia with non-obstructive coronary arteries. aIn selected patients. bConsider also coronary spasm or microvascular dysfunction.
Key Insights Cracking the Code on Chronic Coronary Syndromes:
When it comes to coronary artery disease (CAD), symptoms of myocardial ischemia from obstructive atherosclerosis can closely mimic those of coronary microvascular disease (CMD) or vasospasm. Despite differences in how men and women present with CAD, both genders should receive similar guideline-directed preventive treatments. Enhancing classic CAD risk models by
incorporating additional factors can help identify patients with a very low probability of obstructive CAD, suggesting that diagnostic testing might be deferred. Coronary artery calcium scoring (CACS) serves as a straightforward tool to adjust the likelihood of CAD. For diagnosing suspected coronary artery disease, non-invasive imaging techniques are generally preferred, with coronary computed tomography angiography (CCTA) being the go-to for ruling out obstructive CAD, while functional imaging helps assess myocardial ischemia and guide treatment decisions.
When considering interventions, invasive coronary angiography (ICA) is advised for those with a very high likelihood of CAD, severe symptoms, or high event risk. For those with intermediate stenoses, evaluating functional severity through invasive methods (like FFR or iFR) before revascularization is recommended. Current guidelines favor using imaging guidance during complex percutaneous coronary interventions (PCI). Antithrombotic therapy typically involves a single agent like aspirin or clopidogrel for long-term management, but dual antiplatelet therapy (DAPT) may be warranted in high-risk patients. For those undergoing PCI and requiring oral anticoagulation, a combination of anticoagulants and
antiplatelet drugs is advised for a period based on ischemic and bleeding risks. Lifestyle changes, risk factor management, and shared decision-making between patients and healthcare professionals remain critical for effective coronary care. Moreover, improving the diagnosis and treatment of conditions like ANOCA/INOCA and ensuring adherence to healthy behaviors are essential for better long-term outcomes.
References:

