Atrial Fibrillation Redefined: Key Insights From The 2024 Esc Guidelines
Atrial fibrillation (AF) is on the rise, and the 2024 ESC Guidelines are here to tackle it head-on. With AF cases expected to double due to an aging population and better detection, these new guidelines introduce the AF-CARE framework—a game-changing approach to managing this complex condition.
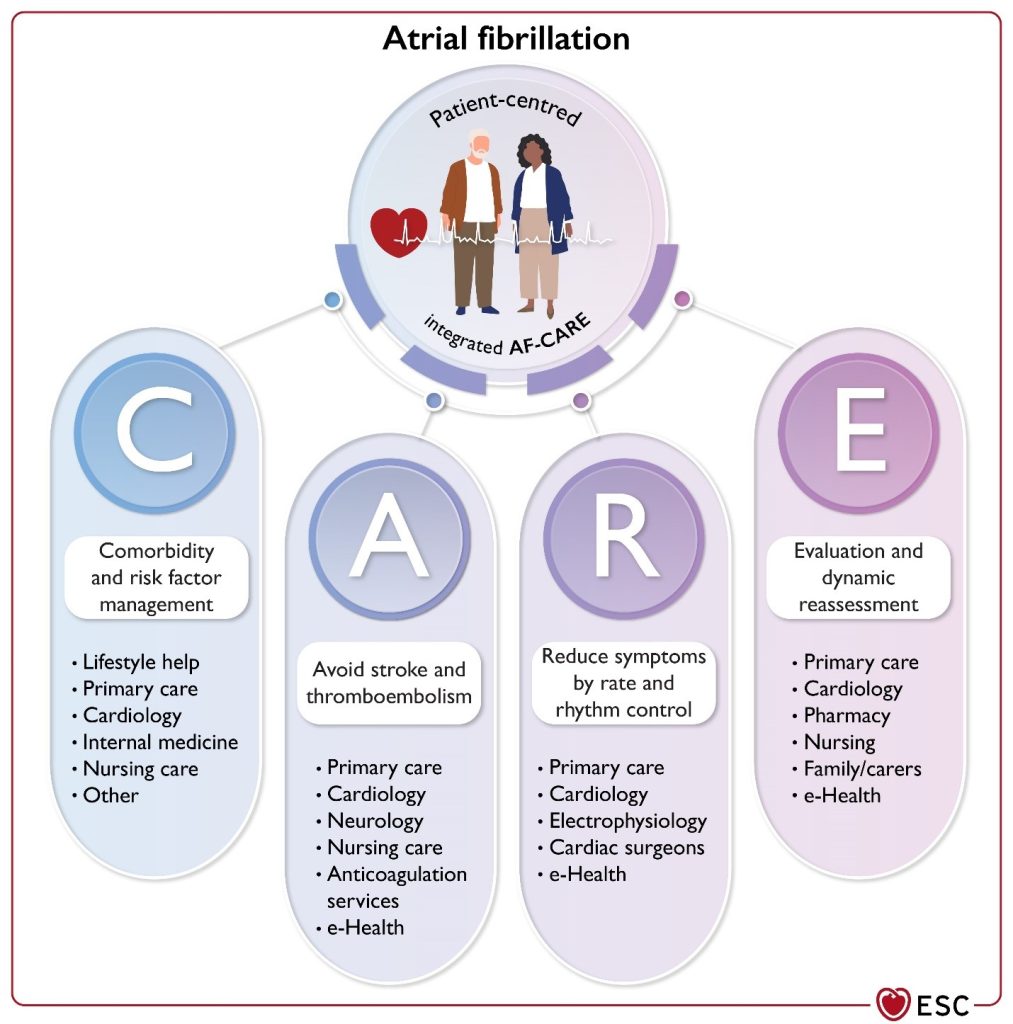
The AF-CARE framework prioritizes a holistic approach: start by managing comorbidities and risk factors, then focus on preventing strokes and blood clots, and finally, control symptoms through innovative treatments. Regular reassessment ensures that care evolves with each patient’s needs.
Empowering patients and fostering shared decision-making are at the heart of these guidelines, aiming to enhance adherence and outcomes. By translating cutting-edge research into practical advice, the 2024 guidelines promise a more effective, patient-centered strategy for managing atrial fibrillation.
Navigating Atrial Fibrillation Management: The Comprehensive Approach
Shared and Equitable Care
A patient-centered approach is key to managing AF, involving joint decision-making and collaboration with a multidisciplinary team. It’s crucial to ensure equal care across different genders, ethnicities, disabilities, and socioeconomic backgrounds. Education for patients, families, caregivers, and healthcare professionals supports informed decision-making and effective management.
Diagnosis and Initial Evaluation
Confirming AF through an ECG is the first step in risk assessment and management. Initial evaluation includes a thorough medical history, symptom impact assessment, blood tests, imaging, and risk factor analysis. Addressing associated conditions like hypertension, diabetes, and obesity is vital for preventing AF progression and improving treatment success.
Anticoagulation Strategy
Oral anticoagulants are recommended for most AF patients to prevent stroke and thromboembolism. Direct Oral Anticoagulants (DOACs) are preferred over Vitamin K Antagonists (VKAs), except in specific cases. Adjustments in dosing and switching between anticoagulants may be necessary based on individual patient risks and control of INR levels.
Balancing Rate and Rhythm Control
For managing symptoms, rate control can be achieved with beta-blockers, digoxin, or calcium channel blockers, depending on the patient's ejection fraction. Rhythm control, including cardioversion and antiarrhythmic drugs, should be considered to alleviate symptoms and improve quality of life, with careful attention to safety and potential interactions.
Advanced Treatments and Ongoing Assessment
Catheter ablation is recommended for persistent or recurrent AF, especially if antiarrhythmic medications fail. In complex cases, endoscopic or hybrid ablation may be an alternative. It’s crucial to perform ablation procedures in specialized centers with experienced teams, particularly during cardiac surgery like mitral valve replacement.
Dynamic and Personalized Care
Regular reassessment of therapy is essential to manage new risk factors and adapt treatment plans. This dynamic approach helps to slow or reverse AF progression, enhance patient quality of life, and prevent adverse outcomes.
Uncovering the Gaps in Atrial Fibrillation Research: Where Future Trials Can Make a Difference
Despite advances in managing atrial fibrillation (AF), several critical gaps in evidence remain that could significantly impact patient care. One major area needing exploration is the definition and clinical relevance of paroxysmal AF, as well as the impact of different durations of AF on treatment outcomes. Additionally, the roles of atrial cardiomyopathy and various comorbidities in AF management are not fully understood, and the influence of diverse factors such as sex, race, and socioeconomic status on AF is still being studied.
Enhancing Patient-Centered Care and Treatment Strategies
The effectiveness of patient education, multidisciplinary care, and remote monitoring in improving AF management remains to be proven. Specifically, the benefits of patient-centered approaches and equal access to care require further validation. There's also a need to establish the role of telemedicine and remote monitoring in the ongoing management of AF.
Improving Comorbidity Management and Anticoagulation Use
Significant gaps exist in understanding how to manage comorbidities such as obesity and sleep apnea in AF patients. While weight loss has shown benefits, consistent methods for achieving it are lacking. Similarly, more evidence is needed on the use of oral anticoagulants (OACs) for various patient subgroups, including those with low stroke risk or complex health conditions. The effectiveness of switching between different anticoagulants and managing anticoagulation post-intracranial hemorrhage also needs further study.
Refining Symptom Management and Rhythm Control
There’s uncertainty about which AF patients truly benefit from rhythm control and how new antiarrhythmic drugs could improve treatment outcomes. Current research suggests mixed results from catheter ablation and cardioversion, highlighting the need for more targeted studies. The effectiveness of various ablation strategies and the value of diagnostic cardioversion in managing persistent AF are areas ripe for exploration.
Optimizing Clinical Settings and Preventive Strategies
In clinical settings, more research is needed to determine the optimal duration of combined OAC and antiplatelet therapy following acute coronary syndrome. The use of direct oral anticoagulants (DOACs) in patients with congenital heart disease and the role of antiplatelet therapy in peripheral artery disease also warrant further investigation. Additionally, there is a need for better risk stratification in AF patients with cancer or those experiencing postoperative AF.
Advancing Screening and Technology Use
Finally, research is needed to evaluate the cost-effectiveness and impact of AF screening strategies, including the use of new consumer devices and wearable technologies. The role of photoplethysmography in screening and the effectiveness of long-term AF detection technologies are still uncertain, highlighting the need for continued innovation and evidence-based practices in AF management.
Figure 1
Multidisciplinary approach to AF management.
Principal caregivers are involved in the community and hospital settings to provide optimal, patient-centred care for patients living with AF. AF-CARE, atrial fibrillation—[C] Comorbidity and risk factor management, [A] Avoid stroke and thromboembolism, [R] Reduce symptoms by rate and rhythm control, [E] Evaluation and dynamic reassessment.
References