


Revolutionizing Heart Failure & Cardiomyopathies Care
“ ESC's 2023 Game-changing Guidelines
This Focus Issue dives deep into the latest advancements and research reshaping the landscape of heart failure and cardiomyopathy management. It introduces new guidelines and reviews recent breakthroughs that are setting new standards in treatment.
The European Society of Cardiology (ESC) has unveiled updated guidelines for managing cardiomyopathies, presenting a fresh approach rather than merely revising previous recommendations. This new framework offers novel insights and strategies, with a specific update to the 2014 guidelines on hypertrophic cardiomyopathy. These guidelines are crafted to provide a comprehensive overview of diagnostic approaches and general management principles, rather than detailed instructions for each cardiomyopathy subtype.
In parallel, the ESC has also issued a focused update to the 2021 heart failure guidelines, integrating findings from recent clinical trials up to March 2023. This update is crucial for adapting treatment strategies based on the latest evidence, bridging the gap until the next comprehensive guideline revision.
A major highlight in heart failure treatment is the role of sodium-glucose co-transporter 2 (SGLT2) inhibitors, particularly for heart failure with preserved ejection fraction (HFpEF). Landmark trials such as DELIVER and EMPEROR-Preserved have confirmed that SGLT2 inhibitors can significantly reduce hospitalizations and cardiovascular deaths. These medications improve cardiac function through a range of mechanisms, including enhancing energy metabolism, reducing inflammation, and modifying nutrient sensing and iron homeostasis. They also lower epicardial adipose tissue and impact adipokine signaling, further supporting their role in HFpEF management.
A viewpoint article emphasizes the need to address coronary artery disease (CAD) in heart failure with reduced ejection fraction (HFrEF). While current therapies effectively manage the secondary effects of reduced cardiac contractility, there is a growing recognition of the importance of preventing recurrent myocardial injury. The management of CAD and restoration of coronary blood flow could potentially improve left ventricular systolic dysfunction, though there is a surprising lack of clinical trials specifically evaluating this approach in HFrEF patients.
Figure 1
The upper part of the figure shows the characteristics of the included RCTs at the sides, and the pulmonary artery sensor, patient electronics system, and the pulmonary artery pressure database in the middle. In the lower part of the figure, the x-axis presents the risk ratio, the y-axis presents the data points of clinical endpoints as addressed, the dot is the point estimate of the hazard ratio pooled estimate, and the bars correspond to the 95% confidence interval. CI, confidence interval; EF, ejection fraction; HR, hazard ratio; HF, heart failure; HFH, heart failure hospitalization; M, months; NT-proBNP, N-terminal pro-B-type natriuretic peptide; NYHA, New York Heart Association; PA, pulmonary artery
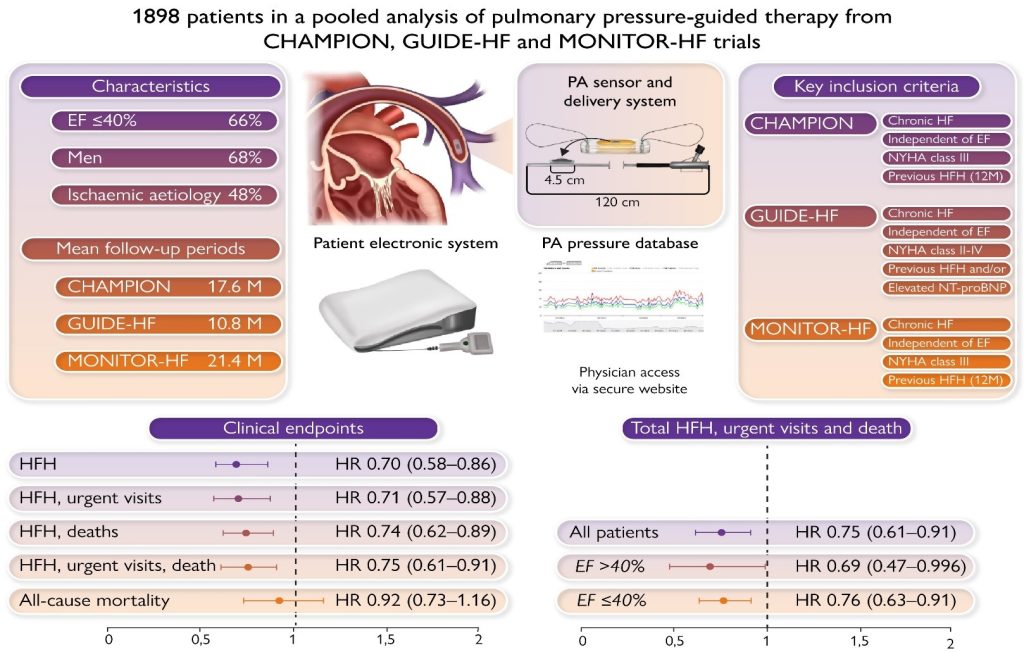
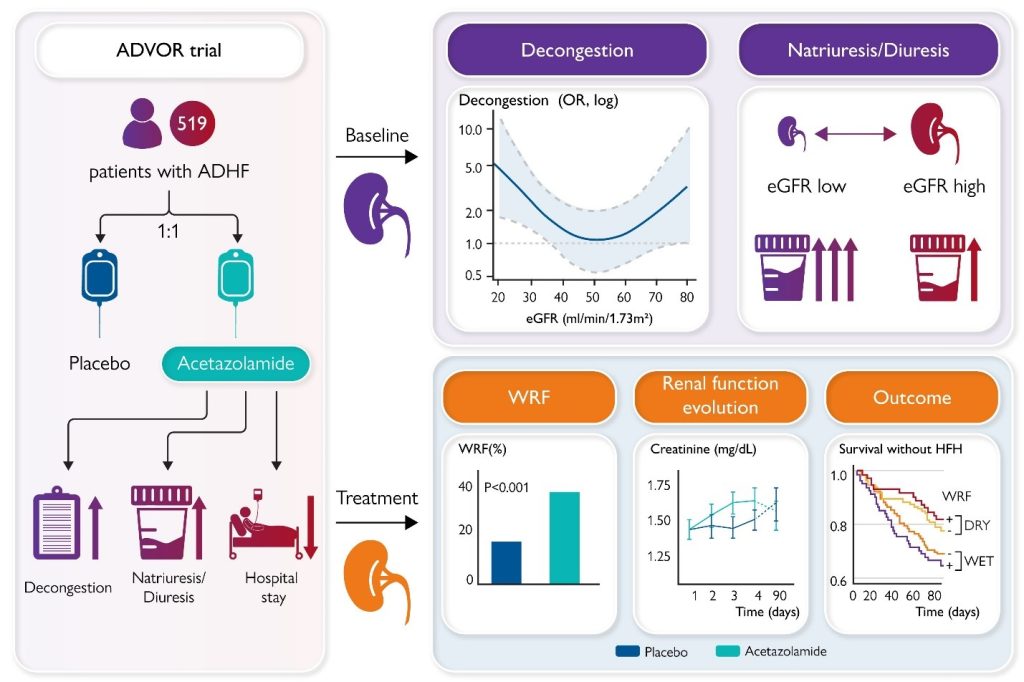
Figure 2
ADHF, acute decompensated heart failure; eGFR, estimated glomerular filtration rate; HFH, heart failure hospitalization; OR, odds ratio; WRF, worsening renal function

